

Short answer: CMS published guidance for the responsible use of AI inside its own operations. It does not regulate vendors, though it sets a clear bar for what trustworthy clinical AI looks like: a qualified human stays in the loop, patient data stays protected, the system shows its reasoning, and every decision is documented. For any executive evaluating an AI tool, those four principles double as a buying checklist.
Artificial intelligence stopped being a boardroom hypothetical a while ago. It is in your documentation workflows, your revenue cycle, and the pitch decks landing in your inbox every week. The harder question for a CEO, CFO, or COO is no longer whether to adopt AI. It is how to tell a defensible AI investment from an expensive one.
That is where a quiet government document becomes useful. CMS recently updated its guidance for the responsible use of AI, and while it was written for CMS staff and contractors, it gives healthcare leaders something they rarely get: a credible, vendor-neutral definition of what “good” looks like.
What is the CMS AI guidance?
The CMS guidance for responsible use of AI is an internal policy governing how CMS employees, contractors, and partners develop and use AI when handling sensitive data. It draws on the NIST AI Risk Management Framework and 2025 federal directives, including OMB memos M-25-21 and M-25-22.
It is internal governance rather than regulation. It does not bind every healthcare AI vendor the way HIPAA does. Its value to you is as signal. When the agency that sets the tone for American healthcare writes down how it expects AI to behave, it tells the rest of the market where the ground is shifting.
Why should healthcare executives care about internal CMS rules?
Because adoption is running ahead of oversight, and the gap is now a board-level risk.
A Sage Growth Partners survey found that only 13% of hospital C-suite executives said their organization had a clear strategy for integrating AI into clinical workflows, and nearly 70% cited data privacy and security as a major obstacle. The pilot era is ending. The next measure of success is whether a system can be governed, audited, and trusted.
The CMS guidance matters to executives for three practical reasons:
- It gives you a yardstick to evaluate vendors that did not come from a vendor.
- It previews the direction of future regulation and payer expectations.
- It signals the documentation and oversight your own teams will be expected to maintain.
The principles CMS expects from responsible AI
Read past the procedural language and a consistent philosophy emerges. CMS expects AI that is:
- Human-supervised. AI provides advice and recommendations. A qualified person makes the final call in consequential cases, with documented oversight. The tool informs the decision. It does not become the decision-maker.
- Data-protective. Sensitive data, including PHI and PII, stays out of public AI tools and inside controlled, authorized environments. Access is limited to what the task actually requires.
- Validated before trusted. Teams are told never to rely solely on AI output. Every result is checked against trustworthy sources and expert judgment before it informs a decision.
- Transparent. AI use is disclosed, sources are cited, and the reasoning behind an output is documented so it can be traced and questioned.
- Documented and auditable. Prompts, model configurations, datasets, and monitoring activity are recorded and versioned so a system can be reviewed, reproduced, and improved over time.
None of these are exotic. Together they describe a particular kind of AI: governed, auditable, privacy-respecting, and built to support expert humans.
How to use these principles when evaluating an AI vendor
Here is the part worth bringing into your next vendor conversation. The CMS principles translate cleanly into questions that separate production-grade clinical AI from a polished demo.
- Where does a human make the final call? If the tool generates orders or determinations on its own, your liability exposure goes up. Confirm where clinician judgment sits in the workflow.
- Where does our patient data live? Ask whether PHI ever leaves your environment, whether it is used to train the vendor’s models, and whether on-prem or containerized deployment is available.
- Can the system show its reasoning? Avoid black-box tools. A clinician or auditor should be able to see why a recommendation was made and which source rules or data produced it.
- What is the evidence? Ask for external validation across multiple sites and peer-reviewed studies, not internal accuracy metrics alone. Strong lab numbers routinely collapse in real-world use.
- How do you handle model drift? AI performance degrades over time. Confirm how the vendor monitors, versions, and corrects it after go-live.
- Does the contract transfer clinical liability? Usually it does not. Read the indemnification and liability terms closely before assuming risk has moved off your books.
A vendor that answers these clearly is building toward the same bar CMS is setting. A vendor that cannot is asking you to be the test case.
Where the next decade of value sits
Payer reality becomes a clinical input at the front of the encounter instead of a billing cleanup task at the end of it, which is the foundation of real denial prevention.
The system then learns from every outcome, reinforcing the patterns that get approved and correcting the ones that get denied, so the clinical reasoning sharpens with each cycle. This is deliberately complementary to the scribe market. The scribe vendors are very good at what they do, and choosing among them is a decision each health system should make on its own EHR and its own terms. cliexa operates on the output, turning a captured record into a defensible decision. The scribe era solved capture. The value that remains sits one layer up, in the reasoning that converts a record into sound clinical and financial action, and cliexa is built for that layer.
The bigger shift: from backward-looking to forward-looking AI
Most AI in healthcare today looks backward. It summarizes what already happened in a record. That is useful, and it is the easier half of the problem. The harder and more valuable work is reasoning about what should happen next, in a way a clinician can see, question, and stand behind.
That kind of system only earns trust if it is transparent about its reasoning, careful with patient data, and honest about the line between a recommendation and a decision. The CMS guidance is essentially a description of those guardrails. Its arrival is a healthy sign that the field is converging on them.
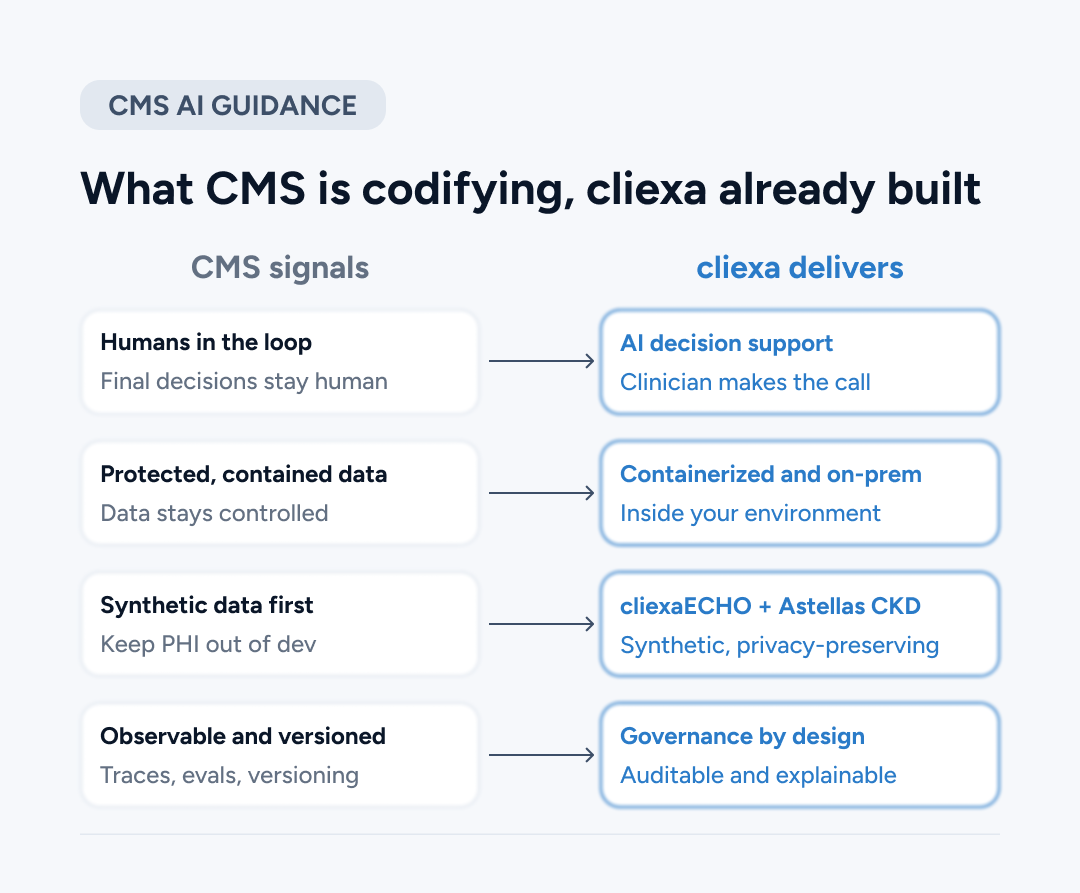
Where cliexa fits
cliexa was built around these convictions before the guidance was written, because they are how responsible clinical AI has to work.
cliexaAI reads payer rules, provider protocols, and the patient’s real-time state, then surfaces what is medically necessary and compliant at the point of care. The clinician sees the reasoning and the source rules and makes the call. Protected health information stays out of development environments, an approach cliexa took to build a chronic kidney disease prediction model with Astellas. Containerized and on-prem options keep sensitive data inside the environments customers already govern. Versioning and explainable, clinically defensible reasoning are part of how the platform is constructed, so a clinical or compliance team can see which version produced a given output and why.
The bottom line
The CMS guidance reads as confirmation of a direction the field is now converging on. Keep humans in charge, keep data protected, show the reasoning, and prove the work. For healthcare leaders, it is also a free evaluation framework. The next time an AI vendor is across the table, the agency that sets the tone for American healthcare has effectively handed you the questions to ask.
Put these questions to us.
The six questions above are the ones we built cliexa to answer. Bring them to a 30-minute walkthrough and see how cliexaAI handles human oversight, data protection, and explainable reasoning at the point of care.
Frequently Asked Questions
What are the core principles of responsible AI in healthcare?
Human oversight of consequential decisions, protection of PHI and PII, validation of AI output against trusted sources, transparency of reasoning, and documented, auditable processes.
What should healthcare executives ask AI vendors?
Where a human makes the final decision, where patient data is stored and whether it trains the vendor’s models, whether the system can explain its reasoning, what external validation exists, how model drift is handled, and whether the contract transfers clinical liability.
What does "human in the loop" mean in clinical AI?
It means AI provides recommendations while a qualified clinician makes the final decision in consequential cases, with that oversight documented. The AI supports judgment rather than replacing it.